

In new research, Renuka Diwan, Paul Eliason, Riley League, Ryan C. McDevitt, James W. Roberts, and Jetson Leder-Luis investigate how Medicare’s shift to a competitive bidding system to reduce prices has inadvertently shifted market share to fraudulent suppliers.
Governments frequently turn to competitive markets to reduce the costs of delivering public goods and services. For instance, with procurement auctions, which require suppliers to bid in order to win contracts, competitive bidding is intended to reduce prices and limit the potential for excessive profits. For markets susceptible to fraud, waste, and abuse, such as durable medical equipment or non-emergent ambulance rides, these lower prices—and the corresponding lower profits—may also reduce the incentives for fraudulent firms to engage in illicit behavior if competitive bidding makes the market a less lucrative target.
Competition can have the opposite effect, however, if fraudulent firms have lower costs because they cut corners, evade compliance, or inflate claims without losing substantial business. While price reductions may ostensibly save the government money, they may also compress margins to the point where legitimate firms can no longer operate profitably. In that case, competitive bidding may inadvertently reallocate market share towards suppliers willing to behave unscrupulously.
In our new paper, we examine the theoretical tradeoff between reducing prices and increasing fraud in Medicare’s procurement of durable medical equipment (DME). We show that although competitive bidding substantially reduced prices and total spending, it also increased the market share of fraudulent firms by driving out legitimate suppliers that could not match their crooked rivals’ artificially low costs.
Medicare’s DME Program
Medicare spends roughly $10 billion annually on DME, including oxygen equipment, wheelchairs, hospital beds, and CPAP machines. Before 2011, suppliers were reimbursed using a regulated fee schedule, with rates based on historical charges that in many cases were viewed as overly generous, often resulting in high profit margins that proved enticing for fraudulent suppliers. As a result, improper payment rates for DME hover around 20 percent of the total payment due to schemes like billing for equipment that never gets delivered, providing equipment to patients who lack a medical need for it, upcoding claims to more expensive equipment, and supplying low-quality equipment while billing at higher reimbursement rates. Because Medicare cannot evaluate every patient for medical necessity or inspect each piece of equipment, this fraudulent activity was difficult to stop.
In response to the outsize levels of spending and fraud, Medicare piloted a series of procurement auctions in several waves across different metropolitan areas and product categories, forcing suppliers to compete with one another by submitting bids to serve a region, with the reimbursement price set at the median of the winning bids. Prior work has shown that the auctions substantially reduced prices and total spending but not how they affected fraudulent behavior.
Competition reduced spending, but not uniformly
We identify fraud across suppliers in two ways. First, we identify sanctioned firms using enforcement data from Department of Justice press releases and the Office of Inspector General’s list of excluded individuals and entities. We then identify suspicious firms that have ties to sanctioned firms through shared ownership, addresses, or referral networks. Throughout the analysis, we group sanctioned and suspicious firms together and categorize them as “fraudulent.”
Using the staggered rollout of competitive bidding across markets and product categories, we then estimate difference-in-differences regressions that compare treated and untreated markets over time. We find that after initiating procurement actions, payments to legitimate suppliers declined by nearly 46 percent, whereas payments to fraudulent suppliers fell by only a third as much, at 14 percent. Claims submitted by legitimate firms to Medicare also dropped sharply, while those from fraudulent firms increased.
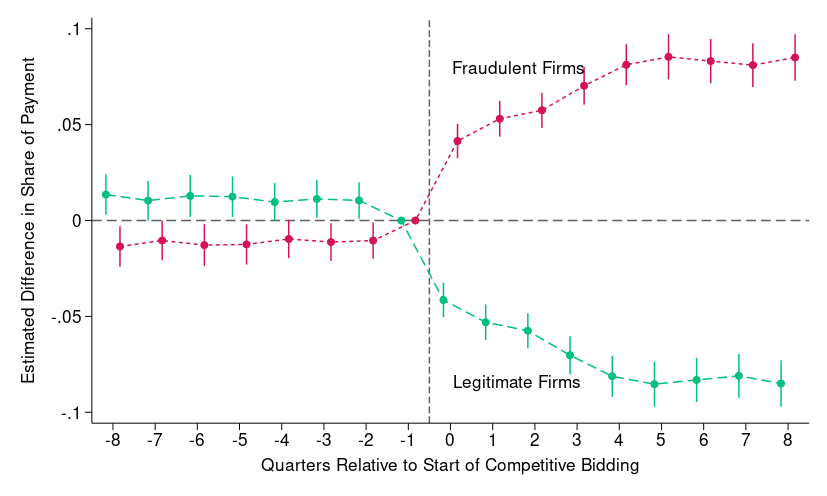
As a result, the market shares of DME suppliers shifted considerably: fraudulent firms’ increased by approximately 8.1 percentage points after the start of competitive bidding, with a corresponding decline for legitimate firms. This divergence began immediately after Medicare’s shift to competitive bidding and has persisted over time, with the overall number of active firms falling due to the disproportionate exit rate of legitimate suppliers. In short, price competition reduced spending primarily by driving out legitimate firms, while fraudulent firms substantially increased their share of the market.
Figure 1: Effect on DME Payment Market Share by Firm Type
Why did fraudulent firms gain market share?
Fraudulent firms have lower effective costs for various reasons: they bill for equipment that never gets delivered, inflate claims through upcoding, avoid expenditures related to compliance, and provide substandard equipment. Legitimate firms, by contrast, bear the full costs of seeking out eligible beneficiaries, documenting their medical necessity, and supplying them with high-quality equipment. Because it’s expensive for Medicare to monitor fraud and firms with higher costs are the first to exit when prices fall, fraudulent firms have a competitive advantage in procurement auctions in light of their artificially low expenses. Although the patterns we observe are consistent with fraudulent firms having lower costs, we also consider several alternative explanations. First, larger firms may have been better positioned to bear the administrative burdens associated with bidding, and fraudulent firms tend to be larger. Although larger firms did gain more market share, their gains were concentrated among the fraudulent firms.
We also examine bidding behavior directly to determine if fraudulent firms appear to game’ the auctions through insincerely low, bad-faith bids that drive out legitimate competition. Fraudulent firms were more likely to submit bids, but conditional on participation, they were not more likely to submit bad-faith bids. Bid distributions are similar across legitimate and fraudulent suppliers—the difference lies not in strategic low-balling, but in the willingness and ability to operate profitably at lower prices.
Lower prices also may have induced firms to engage in more fraud, as shrinking margins might spur suppliers to cut corners, reduce quality, or bill illicitly to offset lost revenue. We find little evidence of such within-firm changes in behavior. Repair and replacement claims, a proxy for DME quality, remain largely unchanged after competitive bidding, as do patient–equipment matches: beneficiaries’ comorbidity profiles and first-time DME claims following a recent hospitalization stayed constant. The rise in fraudulent firms’ market share therefore does not appear to reflect any change in their behavior.
Taken together, the evidence points to a selection effect as the primary cause of fraudulent firms’ market share gains: competitive bidding favored low-cost suppliers, and fraudulent firms have disproportionately lower costs.
Conclusion and policy implications
Our results highlight a broader tension in procurement policy. Competition is commonly perceived as a way to reduce prices and discourage fraud, yet when quality is difficult to monitor and fraud leads to lower costs, competition may favor the firms most willing to cut corners and provide substandard care. In settings with imperfect monitoring, procurement policies and enforcement must complement price competition. Otherwise, cost-based selection may favor suppliers whose low costs reflect misconduct rather than efficiency.
This does not imply that the move to competitive bidding was entirely unsuccessful—it still achieved substantial spending reductions. But it does demonstrate that price reductions alone may not entirely eliminate fraud, and may instead alter market structure in unintended, and undesired, ways.
The relationship between competition and fraud is complex. It depends on the distribution of costs, the ability to monitor quality, and the incentives faced by firms. Medicare’s DME program illustrates how, in markets where fraud reduces the effective costs of suppliers, competition can inadvertently reshape the market in favor of fraudulent firms.
Authors’ Disclosures: McDevitt reports research funding from the American Investment Council, Arnold Ventures, Duke University’s Office of the Provost, the Health Management Academy, the National Bureau of Economic Research, the National Institute for Health Care Management, the National Science Foundation, and the Washington Center for Equitable Growth; he has received consulting fees from the American Society of Nephrology, Korein Tillery, and Charles River Associates, including for matters involving DaVita and Fresenius, as well as speaker fees from Heritage Group, InTandem Capital, and Welsh, Carson, Anderson, & Stowe, and in the past served on the advisory board of Renalogic.
This project received funding from Arnold Ventures under grant 22-08498, and Riley League was supported by the National Institute on Aging, grant number T32- AG000186, while working on this project. He has no other conflicts of interest related to this research.
The other authors report no conflicts of interest. You can read our disclosure policy here.
Articles represent the opinions of their writers, not necessarily those of the University of Chicago, the Booth School of Business, or its faculty.
Subscribe here for ProMarket’s weekly newsletter, Special Interest, to stay up to date on ProMarket’s coverage of the political economy and other content from the Stigler Center.