
In a Facebook post that has since become viral, Italian doctor Daniele Macchini offered a first-hand testimony from the Lombardy region, the epicenter of the epidemic in Italy. He asked readers to share his message “to prevent what is happening here.”
Editor’s note: Daniele Macchini is an Italian doctor working in one of the main hospitals in Bergamo, Lombardy. He wrote a Facebook post to explain what is happening in the epicenter of the coronavirus epidemic in Italy, asking readers “to spread the word to prevent what is happening here.” We translated it into English. Since Macchini wrote this post on March 7, the Italian government has placed most of the economy on lockdown to slow the contagion. High death rates in Lombardy—which has one of the best health care systems in Italy—are probably related to the limited number of intensive care units.
In one of the many emails that I now receive every day from my health department, there was a paragraph entitled “being socially responsible,” with some recommendations that are well worth supporting. After thinking for a long time about it and what to write about what is happening to us, I felt that it would be irresponsible for me to remain silent. So, I will try to convey what we are experiencing in Bergamo during these days of the Covid-19 pandemic.
I understand the need not to create panic, but people are not getting the message about the danger of what is happening. I still hear of people who complain about not being able to go to the gym or to have soccer tournaments. This makes me shudder.
A few weeks ago, I looked with some amazement at the reorganization of my entire hospital. The wards were empty. Intensive care rooms had been freed to create as many beds as possible. This rapid transformation brought to the corridors an atmosphere of surreal silence and emptiness that we had yet to understand. It felt as if we were waiting for a war that hadn’t begun and that many (including me) never expected would come with such ferocity.
I still remember that night shift of mine, a week ago: I was waiting for the outcome of a swab on the first suspected patient in our hospital, thinking about what consequences it would have for us and the clinic. Looking back at it, my agitation that night for one possible case seems almost ridiculous and unjustified now that I have seen what is happening. The situation is now nothing short of dramatic.
One after another, patients come to the emergency room. Usually, the people of Bergamo do not come to the emergency room at all. They followed the doctors’ prescriptions this time too: a week or ten days at home with fever without going out and risking contagion. But when they can no longer breathe enough, they need to come in for oxygen.
Drug therapies for this virus are few. The outcome mainly depends on the patient’s own organism. We can only hope that the body will eradicate the virus on its own, and we merely try to help it in the effort. Staying at home until the symptoms worsen does not change the prognosis of the disease.
One after another, the departments that had been emptied are filling up at an impressive rate. The display boards with the names of the patients, normally of different colors depending on the operating unit they belong to, are now all red. And instead of stating the patient’s surgical operation, there is simply the diagnosis, which is always the same: bilateral interstitial pneumonia.
One after another, the unfortunate poor come to the emergency room. They have anything but flu complications, but let’s stop saying it’s a bad flu.
No flu virus causes such a rapid tragedy. In the classical flu, besides infecting a much smaller population over several months, complications also occur less frequently. It is only when the virus destroys the protective barriers the respiratory tract and allows bacteria normally resident in the upper tract to invade the bronchi and lungs that the classical flu can lead to more serious cases.
COVID-19 causes a banal influence in many young people, but in many elderly people (and not only them) it causes a real SARS because it arrives directly in the alveoli of the lungs and infects them, rendering the lungs unable to perform their normal functions. The resulting respiratory failure is often serious. After a few days, the simple oxygen that can be administered in the hospital ward may not be enough.
Sorry, but to me as a doctor, there is nothing reassuring about the fact that the most serious cases are mainly elderly people with other pathologies. The elderly population is the most represented in our country, and it is difficult to find someone who, above 65 years of age, is not already taking medicine for at least high blood pressure or diabetes.
I also assure you that when you see young people who end up in intubated intensive care, pronated or worse in ECMO (a machine for the worst cases, which extracts the blood, re-oxygenates it, and returns it to the body, waiting for the organism, hopefully, to heal its lungs), this reassurance about being young will cease.
There are still people on social networks who pride themselves on being unafraid and ignoring the warnings, complaining that their normal lifestyle habits are “temporarily” in crisis. Meanwhile, an epidemiological disaster is taking place.
There are no more surgeons, urologists, orthopedists: We are only doctors who have suddenly become part of a single team to face this tsunami that has overwhelmed us. The cases multiply, people arrive at the rate of 15-20 hospitalizations a day, all for the same reason.
The results of the swabs now come one after the other: positive, positive, positive. Suddenly the emergency room is collapsing. Emergency provisions are issued: Help is needed in the emergency room. A quick meeting to learn how the first aid management software works, and a few minutes later these specialists are already downstairs, next to the warriors on the war front.
The screen of the PC with the reasons for admittance is always the same: fever and respiratory difficulty, fever and cough, respiratory insufficiency, etc… Exams, radiology, always with the same phrase: bilateral interstitial pneumonia, bilateral interstitial pneumonia, bilateral interstitial pneumonia. All the new arrivals to be hospitalized. Some are already to be intubated and go to intensive care. For others it is too late…
Intensive care becomes saturated, and where the intensive care rooms come to an end, more are created. Those operating rooms that have now suspended their non-urgent activity become places for intensive care that did not exist before.
I found it incredible how it was possible—or at least I can speak for Humanitas Gavazzeni (where I work)—to put in place in such a short time a deployment and a reorganization of resources so finely designed to prepare for a disaster of this magnitude. And every reorganization of beds, wards, staff, work shifts, and tasks is constantly reviewed day after day to try to give everything, and even more.
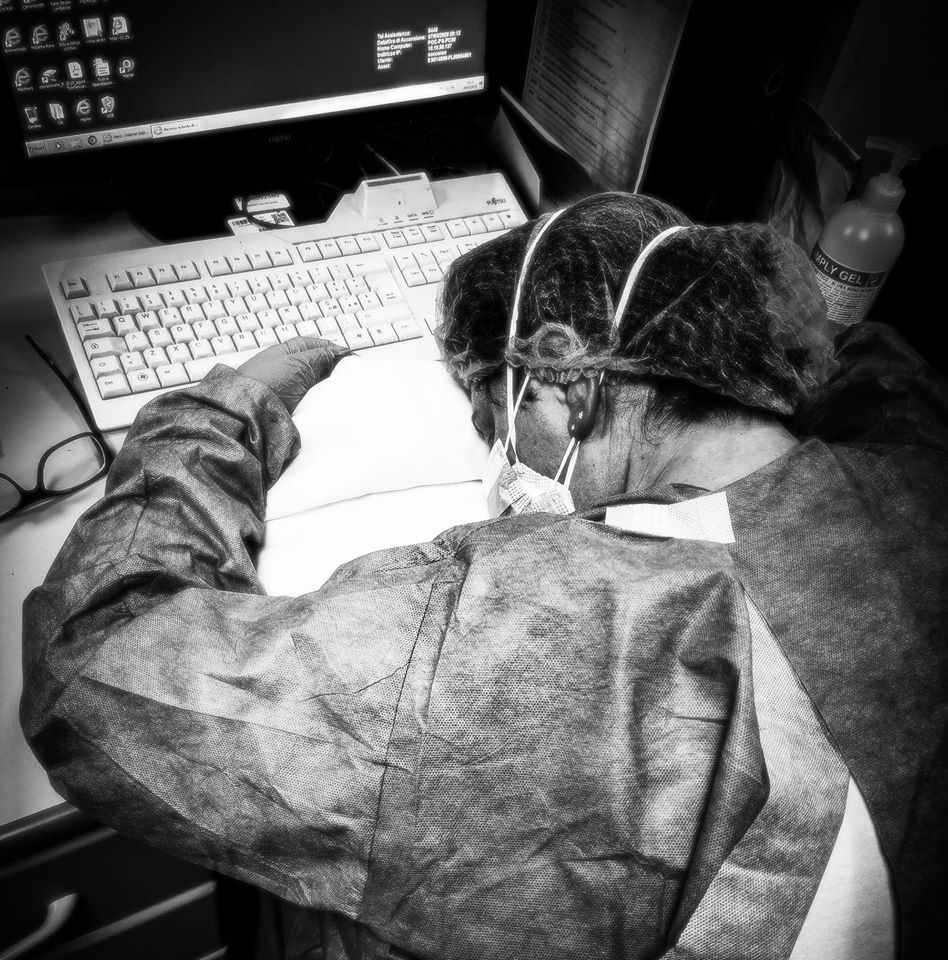
The staff is exhausted. I saw fatigue on faces that never knew what it was despite the already grueling workloads they had. I have seen people work beyond the times they already used to work, for overtime that was now habitual. I saw solidarity from all of us, who never failed to go to our internist colleagues to ask, “What can I do for you now?” or to say, “Leave that hospitalization alone.”
I saw doctors who move beds and transfer patients, who administer care instead of nurses. I saw nurses with tears in their eyes because we cannot save everyone, and the vital signs of several patients at the same time reveal a fate that has already been marked.
There are no more shifts, no more schedules. Social life is suspended for us.
My wife and I separated a few months ago. Since then, I have always done my best to constantly see my son, even on the day of disassembly at night, postponing sleep until when I am without him. But now, for almost two weeks, I have voluntarily not seen either my son or my family for fear of infecting them and infecting an elderly grandmother or relatives with other health problems. I remain content with some photos of my son that I look at in tears, and a few video calls.
So be patient. You can’t go to the theater, museums, or the gym. Try to have mercy on that myriad of older people you could exterminate. It is not your fault, I know. It is the fault of those who put it in your head that we medical professionals are exaggerating. Even this testimony may seem like an exaggeration for those who are far from the epidemic. But please, listen to us. Try to leave the house only to do things that are absolutely necessary.
Do not go en masse to supermarkets to stockpile supplies: It is the worst thing because you concentrate and risk contact with infected people who do not even know they are infected. You can go shopping as you usually do. Maybe if you have a normal mask (even those that are used to do certain manual work), put it on. Don’t look for ffp2 or ffp3. Those should serve us, and we are struggling to find them. By now we have had to optimize their use only in certain circumstances, as the WHO recently suggested in consideration of the almost ubiquitous impoverishment of those supplies.
Due to the shortage of certain devices, I and many other colleagues are certainly exposed, despite all the means of protection we have. Some of us have already become infected, despite the protocols. Some infected colleagues also have infected relatives, and some of their family members are already struggling between life and death.
We doctors work in the very places that others stay away from out of fear. Try to make sure you stay away. Tell your family members who are elderly or with other illnesses to stay indoors. Bring them the groceries, please.
We have no alternative. It is our job. Well, what I have been doing these days is not the job I am used to, but I do it anyway, and I will like it as long as it adheres to the same principles: to try to make some sick people feel better and heal, or even just to alleviate the suffering and the pain of those who unfortunately cannot heal.
Please share and re-share the message. We must spread the word to prevent what is happening here in Italy.
ProMarket is dedicated to discussing how competition tends to be subverted by special interests. The posts represent the opinions of their writers, not necessarily those of the University of Chicago, the Booth School of Business, or its faculty. For more information, please visit ProMarket Blog Policy.